Hypoxemia during intubation has long been associated with increased morbidity and mortality. We have had constant struggle to determine the best way to combat peri-intubation hypoxemia. The reality is each patient presents their own oxygenation challenges and may require different approaches. However, one constant is that preoxygenation/denitrogenation is essential for all patients undergoing RSI, though the method may vary.
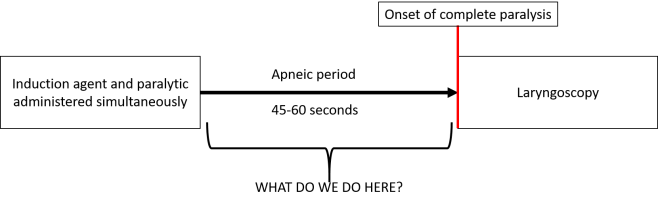
The area of debate has been: how do we handle to apneic period? The primary reason RSI was developed was to prevent aspiration. Therefore, in a customary RSI, no positive-pressure ventilation is provided between induction agent/paralytic administration and laryngoscopy. This is to reduce chances of insufflating the stomach and causing regurgitation. However, many airway experts say their personal practice is to provide gentle BVM ventilation during the apneic period. Some say it is for oxygenation, some say it is more for them to prove the patient can be ventilated should intubation be unsuccessful. These opposing viewpoints have existed without high quality evidence either way, until now.
PreVent was a randomized controlled trial performed in seven ICUs in the U.S. They enrolled 401 patients undergoing endotracheal intubation to receive either no positive-pressure ventilation (n=202) or gentle BVM ventilation during their apneic period (n=199). The two groups were remarkably well balanced. The primary outcome was the lowest oxygen saturation from induction to two minutes after intubation.
In the no ventilation group, the median lowest oxygen saturation was 93% vs. 96% in the BVM group. 45 patients (22.8%) in the no ventilation group had severe hypoxemia, defined as oxygen saturation less than 80%, versus 21 patients (10.9%) in the BVM group. These results were all statistically significant. Perhaps more interestingly though, there was no difference in the rate of operator reported aspiration or new opacities on chest x-ray between the two groups.
The authors concluded that BVM ventilation resulted in higher oxygen saturations and lower rates of severe hypoxemia than no ventilation.
Participants received training in BVM ventilation prior to the study. The guidelines were: proper two handed-mask seal, oropharyngeal airway in place, PEEP valve set to 5-10 cmH2O, ventilator rate of 10 bpm, and tidal volumes only large enough to generate chest rise. These parameters demonstrate excellent BVM technique and are an important aspect to the trial.
This was a well-done study with clinically important results. However, there are some important points to consider when determining if this study should change practice:
-The title of the study was interesting to me. BVM ventilation cannot truly be performed during intubation for obvious reasons. This distinction is important because apneic oxygenation can be performed during the apneic period and throughout the intubation procedure.
-Most of the patients in the study were intubated for respiratory failure (~80%). This represents a patient population who are most likely to be affected by our oxygenation decisions during this time period.
-There were significant differences in how the two groups were preoxygenated. The BVM group was much more likely to have BVM used during preoxygenation (40% vs 11%). The no ventilation group was more likely to receive BiPAP (24% vs 16%) or high flow nasal cannula (20% vs 12%). Overall, the BVM group had more preoxygenation with positive pressure (66% vs 55%). It is difficult to say whether the preoxygenation method would have impacted peri-intubation oxygen saturation. Preoxygenation is likely far more important for preventing desaturation than management of the apneic period.
-The no ventilation group received apneic oxygenation 77% of the time, either with an NRB or nasal cannula, although it was not required in either group. If not ventilating the patient, providing apneic oxygenation seems logical, harmless, and potentially beneficial. The authors also do not specify whether or not the airway was maintained during this time period. Apneic oxygenation is not likely to be effective if airway patency is not maintained with a jaw thrust or airway adjunct. Additionally, the BVM group did not receive apneic oxygenation during laryngoscopy, which may have improved outcomes further. Apneic oxygenation has potential to decrease the rate of desaturation during intubation, but the literature is variable.
-Patients who were judged to be a very high risk of desaturation or aspiration, had hypoxemia, or had academia were excluded. These patients are ones that we care most about when it comes to peri-intubation oxygenation and ventilation so it is difficult to say if these results are generalizable to this population.
-The BVM ventilation performed in this study, at least superficially, seems to have been excellent. The guidelines and training were rigid and show that the authors understood the importance of ensuring high quality BVM ventilation to accurately assess the intervention. Unfortunately, this quality of BVM ventilation does not exist commonly in clinical practice. When ventilating during the apneic period, the risk will be greatly increased if poor technique is used.
-The median time from induction agent administration to laryngoscopy in the BVM group was 98 seconds (range 65-135) and 72 seconds (range 52-120) in the no ventilation group. These times are likely longer than typically seen in clinical practice, although most providers are not accurately timing this period so it is difficult to say. The fact that the BVM group had a longer time to laryngoscopy and still had less desaturation supports the conclusion.
-Three of the seven sites used Mapleson F circuits for bag-mask ventilation. These are quite different than a traditional BVM but are likely effective if used by experienced providers. Post from EMCrit on these devices here:
https://emcrit.org/emcrit/what-the-heck-is-a-mapleson-b-circuitu-probably-shouldnt-care/
-Etomidate or propofol were used as the primary induction agent in about 90% of the patients. At induction doses, these drugs are both likely to cause apnea shortly after administration. It is possible that ketamine allows spontaneous respiration for a longer period of time after administration and before onset of paralysis. Since ketamine has become a primary induction agent in the emergency setting, it would be interesting to see if the results would be different had it been used more frequently.
Is this generalizable to the emergency setting?
Since this study was done in ICUs, it is important to determine if the results can be applied to the ED and prehospital setting. One major factor impacting this is whether or not these patients had eaten full meals recently or had been receiving TPN. I could not find anywhere where they address recent food intake in the manuscript. In the emergency setting, our patients almost always have a full stomach. This certainly could impact the rate of aspiration. Another factor is duration of hospitalization. The manuscript does not appear to address how long these patients had been admitted. Patients in the ICU may be in different phases of respiratory illness than typically seen in the emergency setting which could theoretically impact outcomes.
My Conclusions
This is a high quality study which addresses a critical issue in emergency airway management. I think it demonstrates that BVM ventilation is, most importantly, safe during the apneic period and is likely beneficial for preventing desaturation.
How should this be applied to practice?
Patients who are at significant risk of desaturation or are at risk of being harmed be apnea should be ventilated during the apneic period prior to laryngoscopy using EXCELLENT BVM technique with a PEEP valve. This decision should be balanced against the potential risk of aspiration (though it was not demonstrated in this study).
Other Pertinent Clinical Points
-The use of a PEEP valve on the BVM is essential in this setting and is beneficial in almost every other situation as well.
-Apneic oxygenation should be utilized during intubation whether the patient is ventilated prior to laryngoscopy or not. It is a no-risk intervention which has potential to prevent desaturation.
-Preoxygenation is essential prior to any RSI, method may vary.
PLEASE check out Dr. Josh Farkas’ post on PULMCrit discussing this paper and reviewing techniques to manage the apneic period aside from using a BVM. This is essential reading.
https://emcrit.org/pulmcrit/pressure-rsi/
PreVent Trial:
https://www.nejm.org/doi/full/10.1056/NEJMoa1812405?fbclid=IwAR1hpFKkF-t5G2QA2V1Xg_b8MCAXA0LkXPKoxZqoWXYR4LqG58AlQAxwSZM
PreVent Supplemental:
https://www.nejm.org/doi/suppl/10.1056/NEJMoa1812405/suppl_file/nejmoa1812405_appendix.pdf
Please contact me with any questions, concerns, or comments
amerelman@gmail.com
![]() @amerelman
@amerelman
Casey JD, Janz DR, Russell DW, et al. Bag-Mask Ventilation during Tracheal Intubation of Critically Ill Adults. N Engl J Med. February 2019:NEJMoa1812405.

[…] The Resus Room: Managing the Apneic Period – The PreVent Trial […]
LikeLike