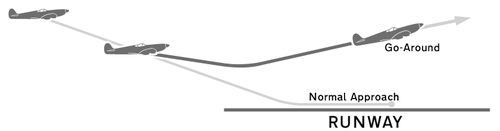
While landing an aircraft, a pilot may decide that the landing has become unsafe or unlikely to be successful. This may be due to a poor approach, another aircraft on the runway, deteriorating weather, or numerous other reasons. Standard procedure in this case is to abort the landing attempt, which involves advancing the throttle to full power, retracting the flaps and landing gear, and establishing a positive rate of climb. The pilot announces to the control tower that they are “going around”. The control tower calmly responds with instructions for the aircraft to set up its repeat approach.
This procedure is well established and commonplace in aviation. As all pilots have, I practiced this procedure many times during my initial flight training and still practice it when I fly. A good pilot is compelled to go around whenever there is any question about the ability to land safely and because of this, a pilot’s decision to do so is never questioned. However, a go-around itself can be dangerous and must be performed properly, as the aircraft is going from low speed into a climb, which increases the risk for stall.
Here is a great video of a go-around. You will hear the ground-position warning system announce “approaching decision height” and then “minimums”. The decision height is the altitude the pilot must decide whether to continue the approach. Minimums indicates that the aircraft is at the altitude where the pilot must be able to visualize the runway to continue the approach.
The pilots had a usable view of the runway and initially continued their approach. Immediately after reaching minimums, the rain became so heavy they could no longer see the runway to continue the landing. They had to make a rapid decision to go around and completely change their mindset from landing to establishing a climb with no visibility, on instruments, and with autopilot off. This is a massive cognitive burden. But there is no panic, argument, or discussion. There is only procedure. These pilots have practiced this before. They know it is the right decision and that no one will criticize it.
In medicine, we have a huge problem admitting when things are not going as planned, especially if we are the ones who made that plan. We worry that we will be scrutinized by others or that we will appear weak.
Imagine a scenario where you are performing a rapid sequence intubation. You are the one intubating and the provider directing the patient care team. You made sure the patient was well prepared, preoxygenated, and hemodynamically supported. You’ve established an oxygen desaturation threshold of 93% to discontinue the attempt. The drugs go in, the patient is paralyzed. You insert the blade as you always do but you don’t see what you are expecting. The epiglottis is visible but it won’t lift. This is the point where your heart rate increases. The moment things begin to deviate from the expected course is the moment situations deteriorate. You try to readjust your blade but the view only worsens. You try to use your Mac as a Miller but can’t see anything after progressing past the epiglottis. You back the blade up again and finally think you can see a sliver of the posterior cartilages, but its not enough. You think you just need to make one final adjustment to have a usable view and someone says, “the sats are 93”.
This is “minimums” in airway management. Do you make that final adjustment to see if it works? Or do you abandon the attempt and ventilate the patient? As with aviation, this decision must be made with safety in mind.
So why is it that so often we reach “minimums” but make the wrong decision? A decision made, not in the name of safety, but out of pride or fear of scrutiny. Or is it because we truly think it is the right thing to do for the patient? This decision is rooted in a culture of task fixation. This culture is instilled in us by our training from day one. How often do we practice abandoning an intubation attempt and reoxygenating a patient? This practice is less about the actual skill and more about how and when to make the go-around decision.
The idea of a go-around is not strictly applicable to airway management. This applies anytime patient care is not going as planned or the patient has a sudden deterioration and requires a rapid change in treatment.
We must:
1. Know and teach how to recognize deteriorating situations or procedures that are unlikely to be successful
2. Know and teach how to respond to these situations, our go-around procedure
3. PRACTICE our go-around procedures as regularly as we practice other treatments
4. Be prepared to change our approach at the drop of a hat if patient safety is at stake
This is about changing culture. We must encourage more go-arounds during resuscitation. Because in many cases, if we don’t go around, patients die.
Here’s what happens when you don’t go around in aviation when you should.

NTSB: “The flight crew did not monitor the descent rate and continued to fly the airplane with a vertical descent rate of 1,500 ft per minute below 1,000 ft above ground level, which was contrary to standard operating procedures, resulting in an unstabilized approach that should have necessitated a go-around.”
Reviewed and edited by Michael Perlmutter
![]() @DitchDoc14
@DitchDoc14
Please contact me with any questions, concerns, or comments
amerelman@gmail.com
![]() @amerelman
@amerelman
